Health Insurance Claim Form Pdf

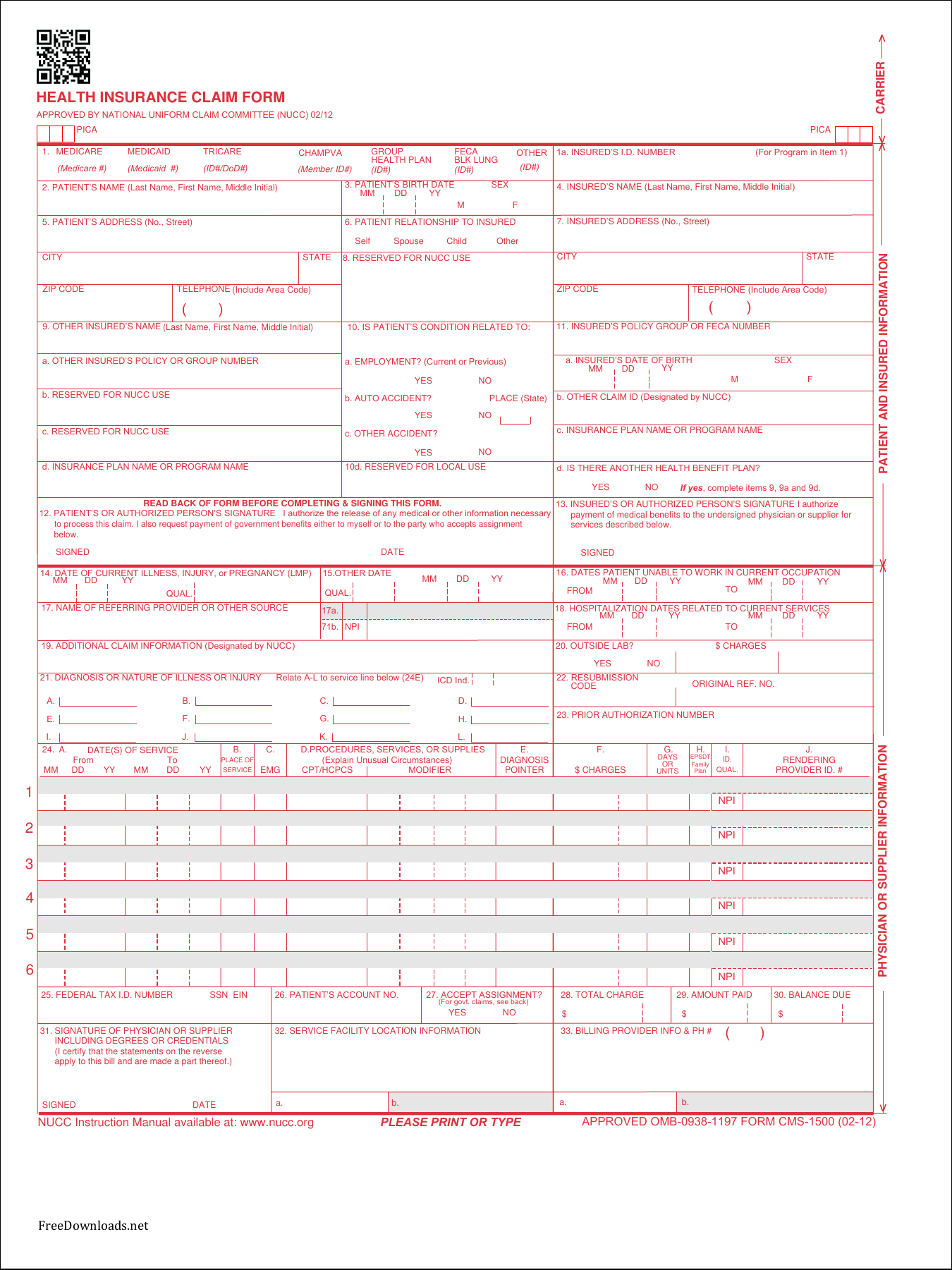

Yes complete items 9 9a and 9d.
Health insurance claim form pdf - Fill out the health insurance claim form online and print it out for free. Hcf contract number 055555 1 i member information. Insurance plan name or program name yes.
Public service health care plan pshcp claim form protected once completed. Is there another health benefit plan. I new tank street valluvarkottam high road chennai 600 034.
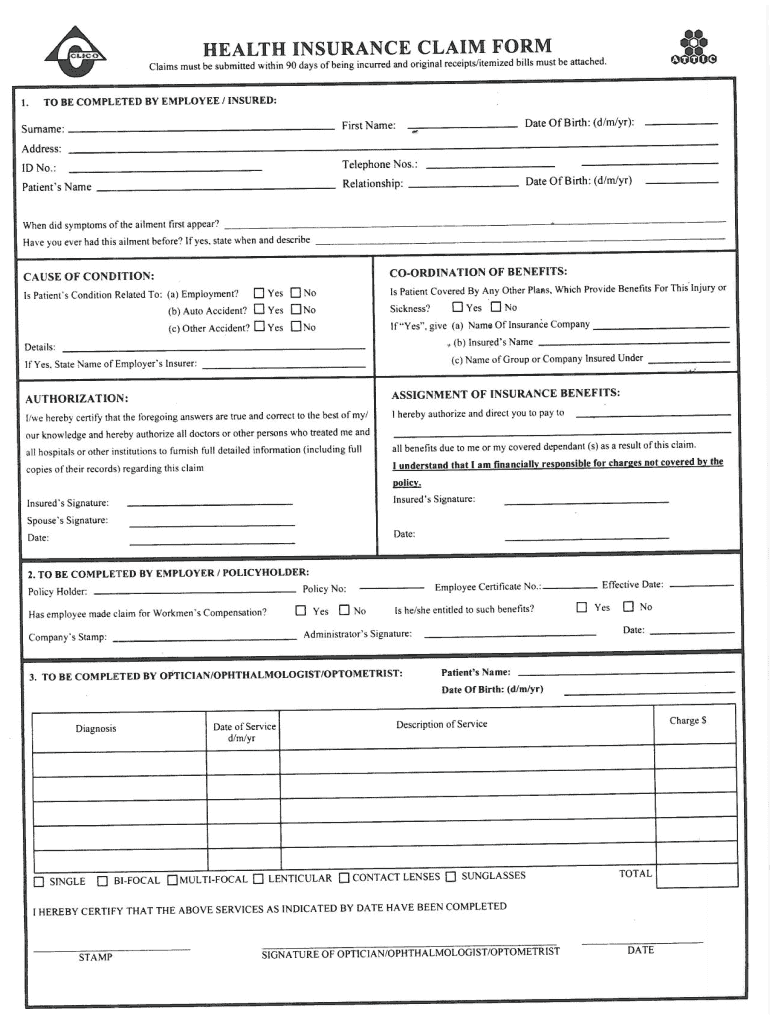
Health insurance product claim form. Health insurance claim form. Request a call back.
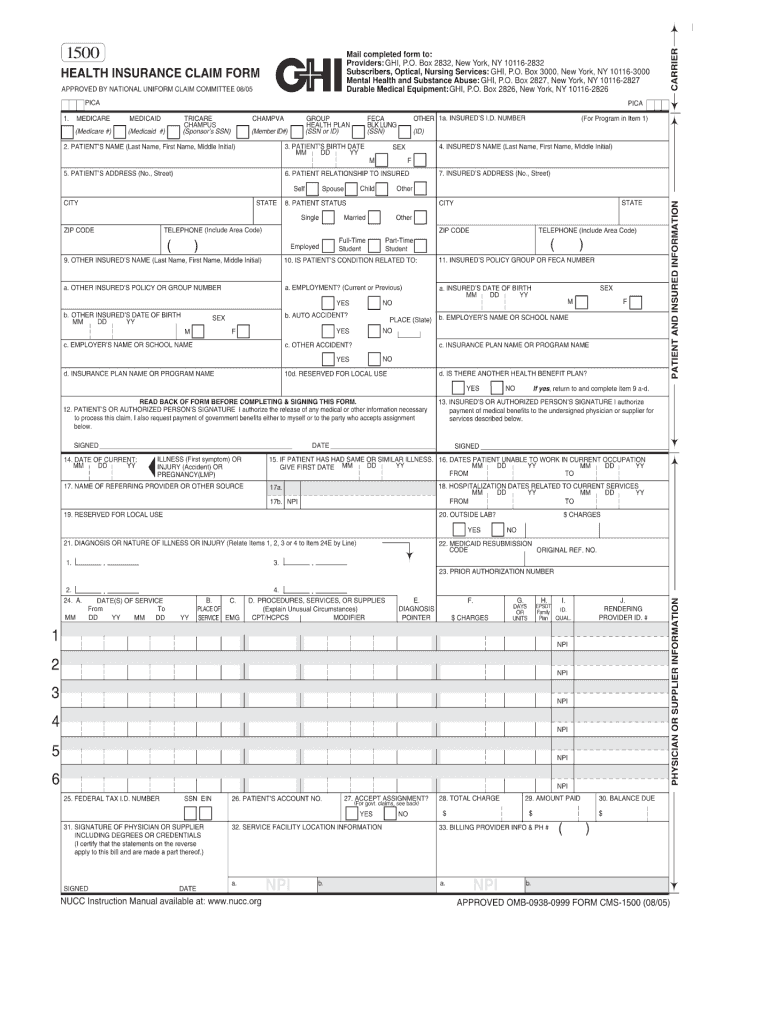
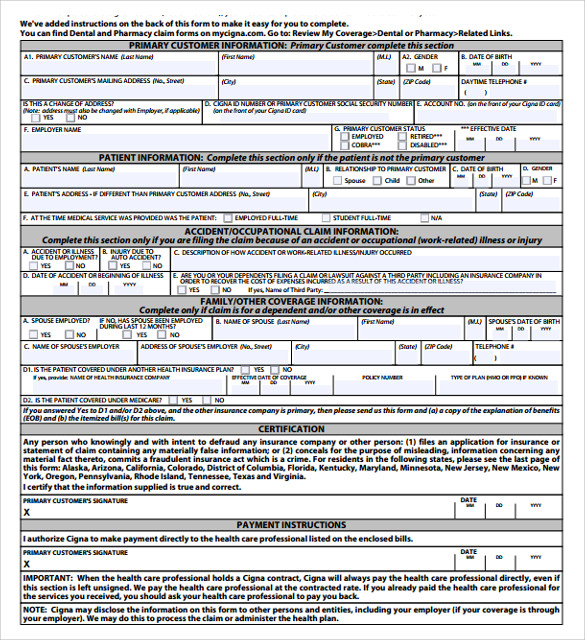
Complete this form if you need to make a health insurance claim and return it with supporting documentation to. Australian unity claims department 114 albert road south melbourne victoria 3205. Department of health and human services centers for medicare and medicaid services united states federal legal forms and united states legal forms.
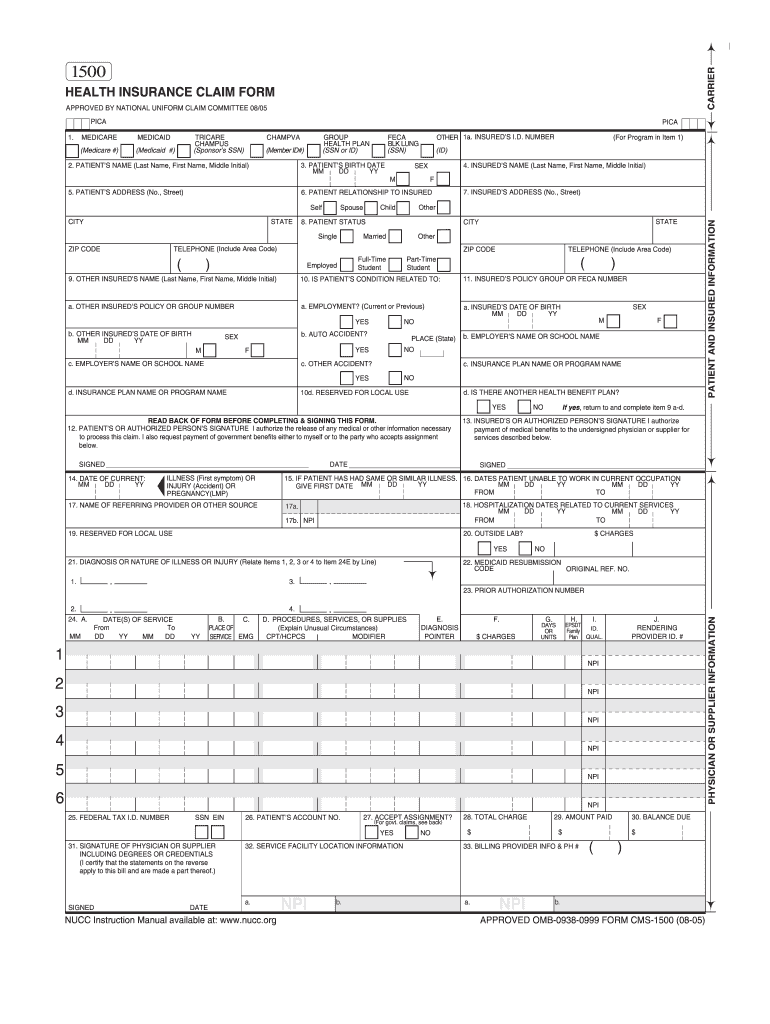
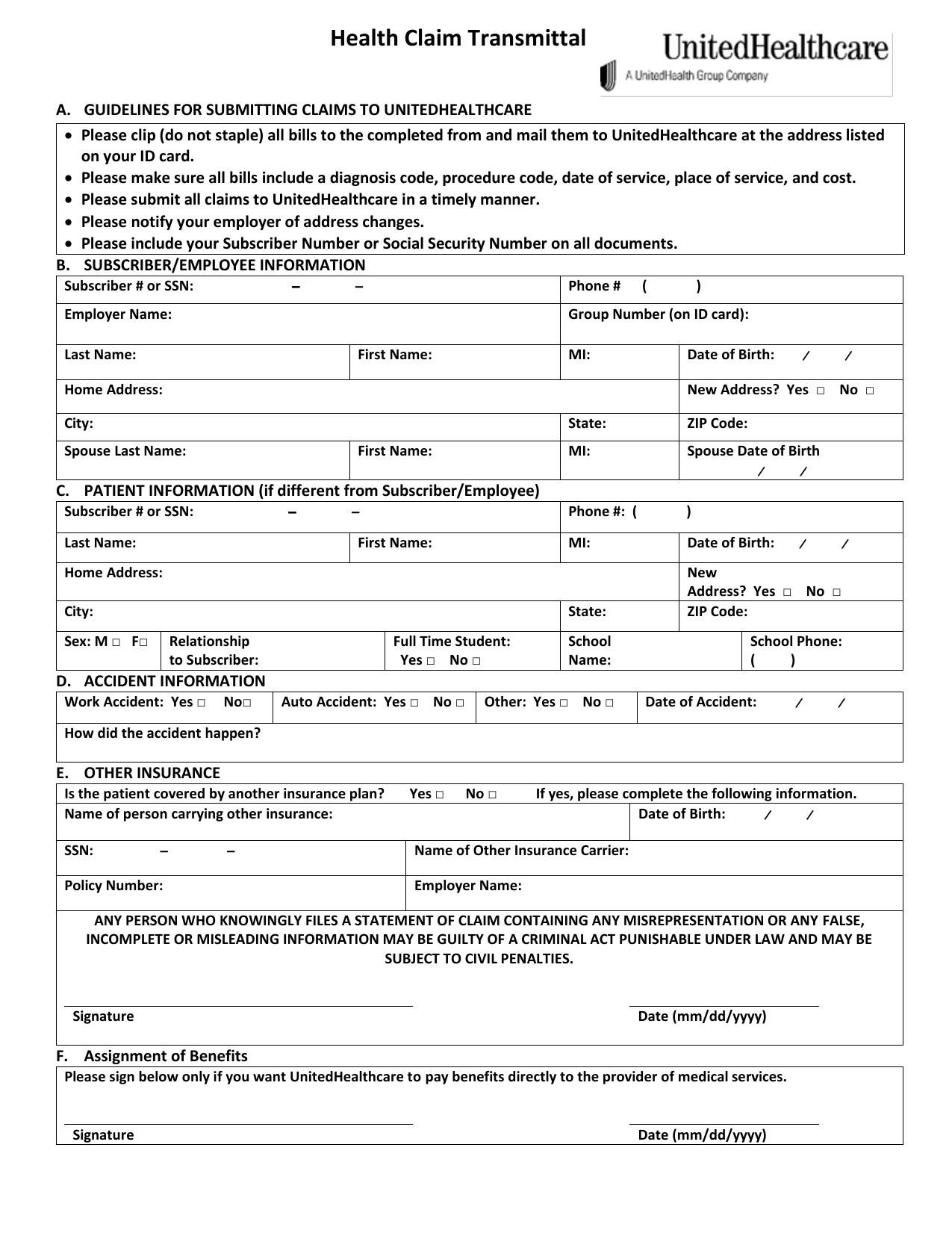
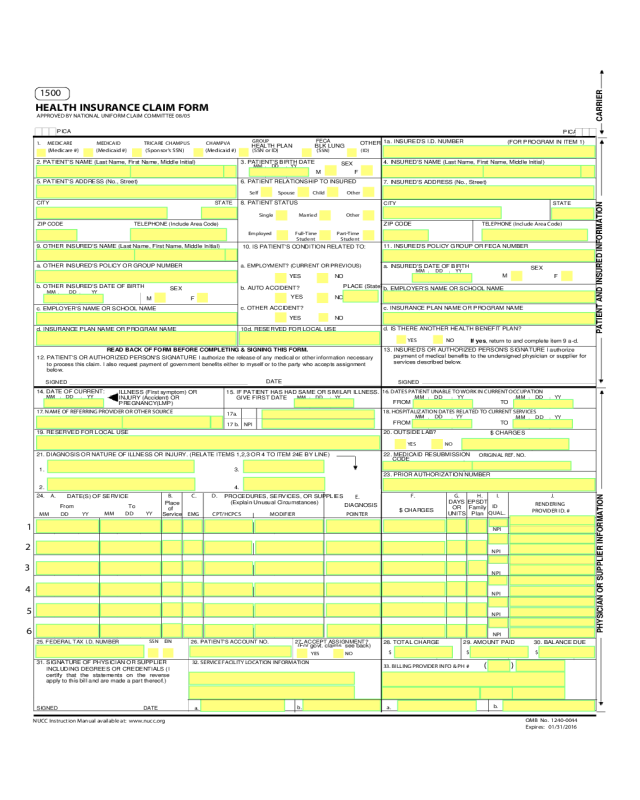
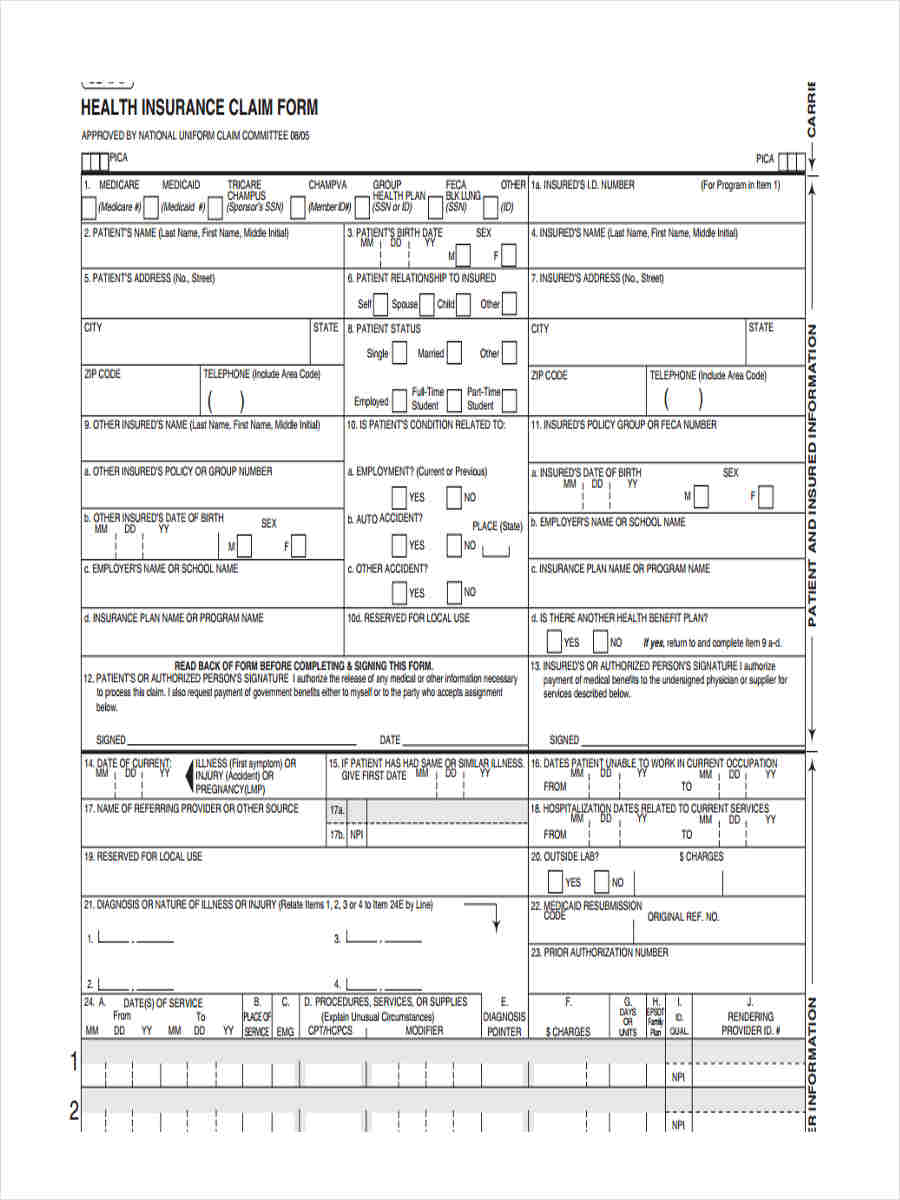
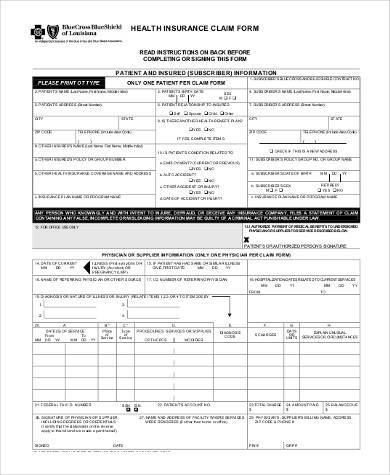
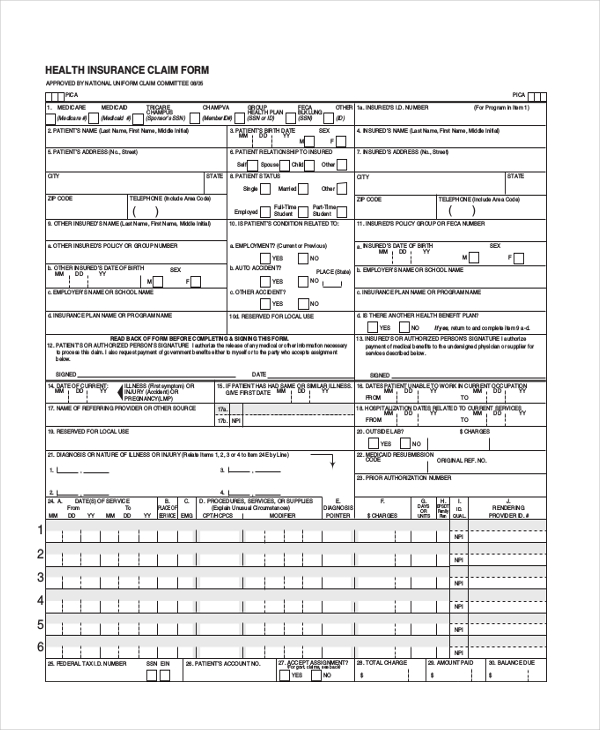
Health insurance claim form 1. Please read all instructions and information. Patient s or authorized person s signature i authorize the release of any medical or other information necessary to process this claim.
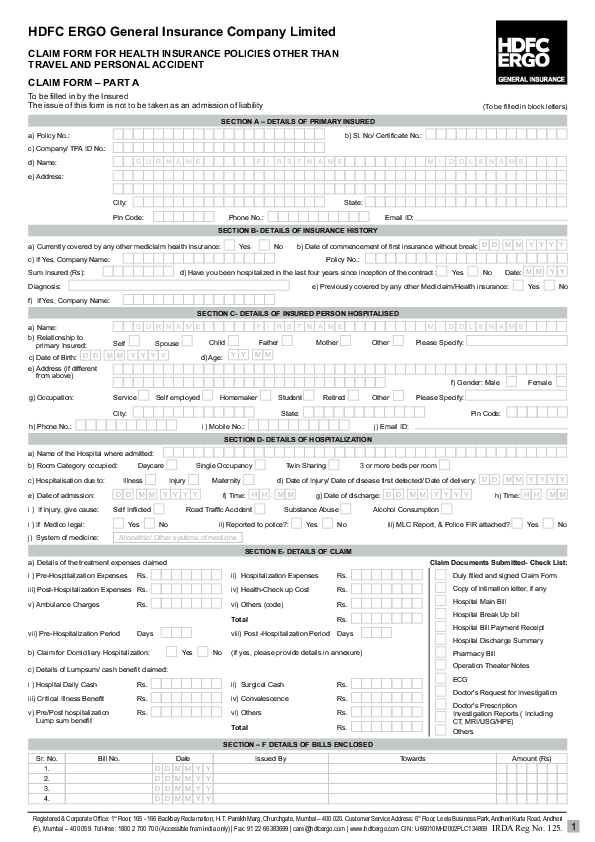
Download the important documents regarding the health insurance claims proposal forms. Star health and allied insurance company limited corporate office. Claim form for medical insurance customer id issuance of this form does not amount to admission of liability under the policy.
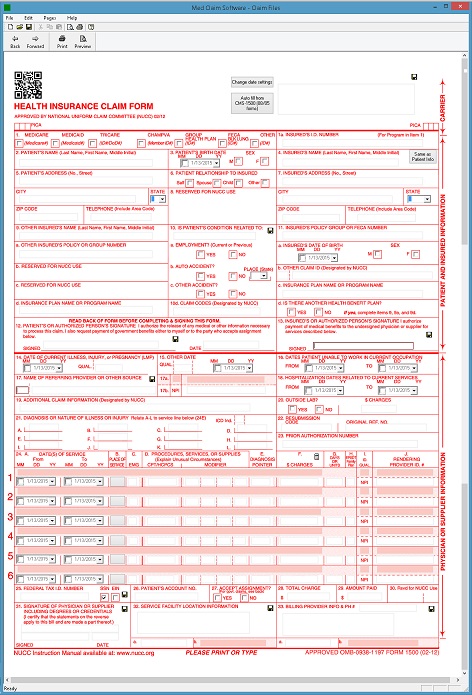
Form 1500 is often used in u s. Corona kavach policy religare health insurance health insurance product pre authorization form. Claim form download the cua health mobile app from apple store or google play for quick and easy extras claiming.
Ce formulaire est disponible en français. Patient s or authorized person s signature i authorize the release of any medical or other information necessary to. Health insurance claim form health insurance claim form 1 of 3 prior approval requires five working days to be processed provided all requested information is submitted.
Make sure that all sections are complete and accurate or this claim will be returned to you. For ho use only. Please be aware that it may be necessary to request further information before completing the assessment for your claim.
Medicare medicaid tricare champva other read back of form before completing signing this form. Other claim id designated by nucc c. I also request payment of government benefits either to myself or to the.
Download printable form 1500 in pdf the latest version applicable for 2020.